Principles of Pharmacology for Medical Assisting 5th Edition Answer Key
ABSTRACT
Since the introduction of insulin analogs in 1996, insulin therapy options for type 1 and type 2 diabetics have expanded. Insulin therapies are now able to more closely mimic physiologic insulin secretion and thus achieve better glycemic control in patients with diabetes. This chapter reviews the pharmacology of available insulins, types of insulin regimens, and principles of dosage selection and adjustment, and provides an overview of insulin pump therapy. For complete coverage of this and related aspects of Endocrinology, please visit our FREE web-book, www.endotext.org.
INTRODUCTION
In 1922, Canadian researchers were the first to demonstrate a physiologic response to injected animal insulin in a patient with type 1 diabetes. In 1955, insulin was the first protein to be fully sequenced. The insulin molecule consists of 51 amino acids arranged in two chains, an A chain (21 amino acids) and B chain (30 amino acids) that are linked by two disulfide bonds (1) (Figure 1). Proinsulin is the insulin precursor that is transported to the Golgi apparatus of the beta cell where it is processed and packaged into granules. Proinsulin, a single-chain 86 amino acid peptide, is cleaved into insulin and C-peptide (a connecting peptide); both are secreted in equimolar portions from the beta cell upon stimulation from glucose and other insulin secretagogues. While C-peptide has no known physiologic function, it can be measured to provide an estimate of endogenous insulin secretion.

Figure 1:
Insulin Structure
SOURCES OF INSULIN
With the availability of human insulin by recombinant DNA technology in the 1980s, use of animal insulin declined dramatically. Beef insulin, beef-pork and pork insulin are no longer commercially available in the United States. The United States FDA may allow for personal importation of beef or pork insulin from a foreign country if a patient cannot be treated with human insulin (2). Beef insulin differs from human insulin by 3 amino acids and pork insulin differs by one amino acid (1).
Currently, in the United States, insulins used are either human insulin and/or analogs of human insulin. The recombinant DNA technique for human insulin involves insertion of the human proinsulin gene into either Saccharomyces cerevisiae (baker's yeast) or a non-pathogenic laboratory strain of Escherichia coli (E coli) which serve as the production organism. Human insulin is then isolated and purified (3-11).
INSULIN ANALOGS
Recombinant DNA technology has allowed for the development and production of analogs to human insulin. With analogs, the insulin molecule structure is modified slightly to alter the pharmacokinetic properties of insulin, primarily affecting the absorption of the drug from the subcutaneous tissue. The B26-B30 region of the insulin molecule is not critical for insulin receptor recognition and it is in this region that amino acids are generally substituted (12). Thus, the insulin analogs are still recognized by and bind to the insulin receptor. The structures of three rapid-acting insulin analogs are shown in Figure 2 (insulin aspart, lispro and glulisine) and the structures of three long-acting insulin analogs are shown in Figure 3 (insulin glargine, detemir, and degludec).
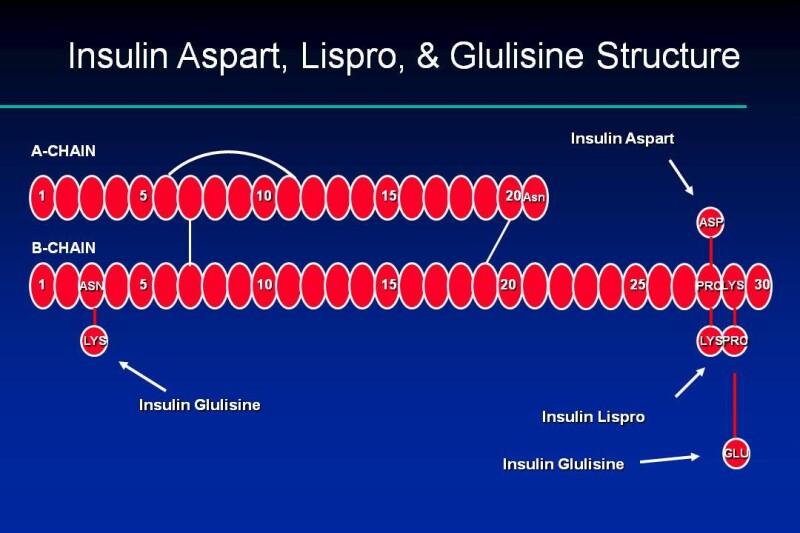
Figure 2:
Insulin Aspart, Glulisine and Lispro Structures

Figure 3:
Insulin Glargine and Detemir Structures
In vitro studies have demonstrated the mitogenic effects of insulin at high concentrations, as well as carcinogenic effects of insulin binding to the insulin like growth factor-1 (IGF-1) receptor, suggesting that hyperinsulinemia may promote tumorogenesis. Because insulin analogs are modified human insulin, the safety and efficacy profiles of these insulins have been compared to human insulin (12). Insulin and IGF-1 receptor binding affinities, and the metabolic and mitogenic potencies of insulin analogs relative to human insulin have been assessed. Insulin lispro and aspart are similar to human insulin on all of the above parameters, except insulin lispro was found to be 1.5-fold more potent in binding to the IGF-1 receptor compared to human insulin. Insulin glargine was found to have a 6- to 8-fold increase in mitogenic potency and IGF-1 receptor affinity compared to human insulin. However, glargine is rapidly degraded to metabolites. The predominant metabolite M1 has been shown to have a 0.4-fold binding affinity to the IGF-1 receptor compared with human insulin (13). In human studies, meta-analyses comparing exogenous insulin to non-insulin antihyperglycemic therapies have shown associations of insulin with several cancers (14,15). However, there are inherent limitations to such analyses. A more recent review of large epidemiologic studies did not find evidence of an increased risk of malignancy among glargine-treated patients when compared with other insulin therapies (13).
Insulin detemir was found to be more than 5-fold less potent than human insulin in binding to IGF-1 (12). An in vitro study showed that insulin degludec had a low IGF-1 receptor binding affinity compared to human insulin (16). The long-term clinical significance of differences in IGF-1 binding among available insulins is not known.
IMMUNOGENICITY
Because pork and beef insulin differ from human insulin by 1 and 3 amino acids respectively, they are more immunogenic than exogenous human insulin. Older formulations of insulin were less pure, containing islet-cell peptides, proinsulin, C-peptide, pancreatic polypeptides, glucagon, and somatostatin, which contributed to immunogenicity of insulin (17). Components of insulin preparations (e.g., zinc, protamine) and subcutaneous insulin aggregates are also thought to contribute to antibody formation (17). Commercially available human insulins are now virtually free of contaminants and contain <1 ppm of proinsulin (1). Local or systemic hypersensitivity reactions, lipodystrophy, and antibody production causing insulin resistance, are now rarely seen with exogenous human insulin (1). Because of the availability of human insulin and the increased potential for animal source insulin to be immunogenic, animal source insulins are no longer available in the United States.
Rare hypersensitivity responses to insulin can be immediate-type, local or systemic IgE-mediated reactions (17). Patients who experience a true allergic reaction to insulin have typically received insulin in the past, and experience the reaction after insulin is restarted.
Delayed, IgG-mediated allergic reactions also develop with animal insulins (17). Insulin therapy can rarely result in the production of insulin antibodies of the IgG class, which inactivate insulin. Immunological insulin resistance can develop in patients with very high titers of IgG-antibodies.
Lipodystrophy resulting from insulin injections refers to two conditions: lipoatrophy and lipohypertrophy. Lipoatrophy is an immune-mediated condition resulting in loss of fat at insulin injection sites (17) and occurs rarely with purified human insulins. Treatment for patients who developed lipoatrophy due to animal insulin use was injection of human insulin into the atrophied site. Lipohypertrophy is a common, non-immunological side effect of insulin resulting from insulin's trophic effects following repeated injections of insulin into the same subcutaneous site (18). Lipohypertrophy can delay the absorption of insulin and therefore it is best if patients do not continue to administer insulin in these locations.
CONCENTRATION
In the United States, all insulins are available in the concentration of 100 units/ml (denoted as U-100). Insulin syringes are designed to accommodate this concentration of insulin. Regular human insulin (Humulin R, Lilly) is available in a more concentrated insulin, U-500 (500 units/ml), and is used primarily in cases of marked insulin resistance, when large doses of insulin (generally > 200 units per day) are required. Extreme caution must be taken as each marked unit on a U-100 syringe will deliver 5 units of insulin. However, syringes specific to U-500 insulin are available, and U-500 insulin is also available for administration via a pen device. For both the syringe and pen specific to U-500 insulin, the units, not the volume, of insulin are marked. Insulin glargine is also available in a U-300 concentration, delivering 300 units/ml, and insulin degludec is available in a U-200 concentration that delivers 200 units/mL. Both U-300 and U-200 insulin are only available in pen devices, and for both U-300 and U-200, the dose of insulin a patient dials into the pen device is in units and not in mL.
Outside the United States, a less concentrated insulin preparation, U-40, (40 units/ml) is still available and sometimes used. Specific U-40 syringes are used with this insulin. It is important that patients traveling from one country to the next be aware of the concentration of insulin they use and that the appropriate syringe is used.
PHYSICAL AND CHEMICAL PROPERTIES
Regular human insulin is crystalline zinc insulin dissolved in a clear solution. It may be administered by any parenteral route: subcutaneous, intramuscular, or intravenous. Insulin aspart, glulisine and lispro are also soluble crystalline zinc insulin, but are intended for subcutaneous (SQ) injection. When administered intravenously, the action of these rapid-acting insulin analogs is identical to that of regular insulin. NPH, or neutral protamine Hagedorn, is a suspension of regular insulin complexed with protamine that delays its absorption. Insulin suspensions should not be administered intravenously. All insulins, except insulin glargine, are formulated to a neutral pH.
Long-acting insulin glargine is a soluble, clear insulin, with a pH of 4.0 which affects its SQ absorption characteristics, discussed further in the pharmacokinetics section. Insulin glargine should not be mixed with other insulins, and should only be administered subcutaneously (7). Insulin detemir is an insulin analog coupled to an 18-chain fatty acid that binds to albumin in the SQ tissue. This results in delayed absorption and a prolonged duration of action. Insulin degludec is an ultra-long insulin analog that breaks down into monomers from dissociating zinc molecules after administration (19). Insulins detemir and degludec should also not be mixed with other insulins and are intended only for subcutaneous use (6,11).
PHARMACOKINETICS
Absorption
Insulin administered via SQ injection is absorbed directly into the bloodstream, with the lymphatic system playing a minor role in transport (1). The absorption of human insulin into the bloodstream after SQ absorption is the rate limiting step of insulin activity. This absorption is inconsistent with the coefficients of variation of T50% (time for 50% of the insulin dose to be absorbed) varying ~ 25% within an individual and up to 50% between patients (1,20). Most of this variability of insulin absorption is correlated to blood flow differences at the various sites of injection (abdomen, deltoid, gluteus, and thigh) (1). For regular insulin, the impact of this is a ~ 2 times faster rate of absorption from the abdomen than other subcutaneous sites (1). The clinical significance of this is that patients should avoid random use of different body regions for their injections. For example, if a patient prefers to use their thigh for a noontime injection, this site should be used consistently for this injection. The abdomen is the preferred site of injection because it is the least susceptible to factors affecting insulin absorption (see Table 1). Insulin aspart, glulisine and lispro appear to have less day-to-day variation in absorption rates and also less absorption variation from the different body regions (3,5,8,21). Insulin glargine's pharmacokinetic profile is similar after abdominal, deltoid or thigh SQ administration (7). Similarly, the glucose-lowering effect of insulin degludec has not been found to vary between abdominal, upper arm, or thigh SQ sites (22).
Factors that alter insulin absorption do so mostly by changing local blood flow in the SQ tissue. Factors that increase SQ blood flow increase the absorption rate. Table 1 lists factors that affect insulin absorption.
Table 1.
Factors Affecting Insulin Absorption (1,12,23)
View in own window
| Factor | Comment |
|---|---|
| Exercise of injected area | Strenuous exercise of a limb within 1 hour of injection will speed insulin absorption. Clinically significant for regular insulin analogs. |
| Local massage | Vigorously rubbing or massaging the injection site will speed absorption. |
| Temperature | Heat can increase absorption rate, including use of a sauna, shower, or hot bath soon after injection. Cold has the opposite effect. |
| Site of injection | Insulin is absorbed faster from the abdomen. Less clinically relevant with rapid-acting insulins, insulin glargine, and insulin detemir. |
| Lipohypertrophy | Injection into hypertrophied areas delays insulin absorption. |
| Jet injectors | Increase absorption rate. |
| Insulin mixtures | Absorption rates are unpredictable when suspension insulins are not mixed adequately (i.e., they need to be resuspended). |
| Insulin dose | Larger doses delay insulin action and prolong duration. |
| Physical status (soluble vs. suspension) | Suspension insulins must be sufficiently resuspended prior to injection to reduce variability. |
Elimination
The kidneys and liver account for the majority of insulin degradation. Normally, the liver degrades 50-60% of insulin released by the pancreas into the portal vein, and the kidneys ~35-45% (21,24). When insulin is injected exogenously, the degradation profile is altered since insulin is no longer delivered directly to the portal vein. The kidney has a greater role in insulin degradation with SQ insulin (~60%), with the liver degrading ~30-40% (25).
Because the kidneys are involved in the degradation of insulin, renal dysfunction will reduce the clearance of insulin and prolong its effect. This decreased clearance is seen with both endogenous insulin production (either normal production or that stimulated by oral agents) and exogenous insulin administration. Renal function generally needs to be greatly diminished before this becomes clinically significant (26). Clinically, a deterioration in renal function leads to a progressive decline in exogenous insulin requirements and an increased risk of hypoglycemia.
PHARMACODYNAMICS
The onset, peak, and duration of effect vary among insulin preparations. Insulin pharmacodynamics refers to the metabolic effect of insulin. Commercially available insulins are categorized as rapid-acting, short-acting, intermediate-acting, and long- acting. Insulins currently available in the United States are listed in Table 2. Insulin pharmacodynamics of the various insulins are shown in Table 3. Ranges are listed for the onset, peak and duration, accounting for intra/inter-patient variability. By having patients self-monitor their blood glucose frequently, the patient-specific time-action profile of the specific insulin can be better appreciated. Figures 4a-4c show the time-activity profiles for available injectable insulins.
Table 2.
Insulins Commercially Available in the US (Recombinant DNA origin)
View in own window
| Category/Name of Insulin | Brand Name (manufacturer) | Preparation(s) |
|---|---|---|
| Rapid-Acting | ||
| Insulin Lispro | Humalog (Lilly) | Vial, cartridge, disposable pen |
| Insulin Aspart | Novolog (Novo Nordisk) | Vial, cartridge, disposable pen |
| Insulin Glulisine | Apidra (Sanofi-Aventis) | Vial, disposable pen |
| Technosphere insulin | Afreeza | Inhaler |
| Short-Acting | ||
| Regular Human | Humulin R (Lilly) Novolin R (Novo Nordisk) | Vial |
| Intermediate-Acting | ||
| NPH Human | Humulin N (Lilly) Novolin N (Novo Nordisk) | Vial, disposable pen Vial |
| Long-Acting | ||
| Insulin Detemir | Levemir (Novo Nordisk) | Vial, disposable pen |
| Insulin Glargine | Lantus (Sanofi-Aventis) Basaglar (Lilly) Toujeo (Sanofi-Aventis) | Vial, cartridge, disposable pen Basaglar is only available as a disposable pen Toujeo is only available as a disposable pen |
| Insulin Degludec | Tresiba (Novo Nordisk) | Disposable pen |
| Insulin Mixtures | ||
| NPH/Regular (70%/30%) | Humulin 70/30 (Lilly) Novolin 70/30 (Novo Nordisk) | Vial, disposable pen Vial |
| Protamine/Lispro (50%/50%) | Humalog Mix 50/50(Lilly) | Vial, disposable pen |
| Protamine/Lispro (75%25%) | Humalog Mix 75/25(Lilly) | Vial, disposable pen |
| Protamine/Aspart (70/30) | Novolog Mix 70/30 (Novo Nordisk) | Vial, disposable pen |
Table 3.
Insulin Pharmacodynamics (3-11,20,23-25,27)
View in own window
| Insulin | Onset (hr.) | Peak (hr.) | Duration (hr.) | Appearance |
|---|---|---|---|---|
| Fast-acting Insulin Aspart A | Within 5 min | ~1 | 3-4 | Clear |
| Insulin Lispro | within 15 min | ~ 1 | 3-5 | Clear |
| Insulin Aspart | within 15 min | 1-3 | 3-5 | Clear |
| Insulin Glulisine | 0.25-0.5 | 0.5-1 | 4 | Clear |
| Technosphere | within 5 min | 15 min | about 3 | Powder |
| Regular | ~ 1 | 2-4 | 5-8 | Clear |
| NPH | 1-2 | 4-10 | 14+ | Cloudy |
| Insulin Detemir | 3-4 | 6-8 (though relatively flat) | up to 20-24 | Clear |
| Insulin Glargine | 1.5 | Flat | 24 | Clear |
| Insulin Degludec | 1 | 9 | 42 | Clear |
| Lispro Mix 50/50 | 0.25-0.5 | 0.5-3 | 14-24 | Cloudy |
| Lispro Mix 75/25 | 0.25-5 | 0.5-2.5 | 14-24 | Cloudy |
| Aspart Mix 70/30 | 0.1-0.2 | 1-4 | 18-24 | Cloudy |
-
Patient specific onset, peak, duration may vary from times listed in table.
-
Peak and duration are dose-dependent, with longer duration of actions seen with large doses.
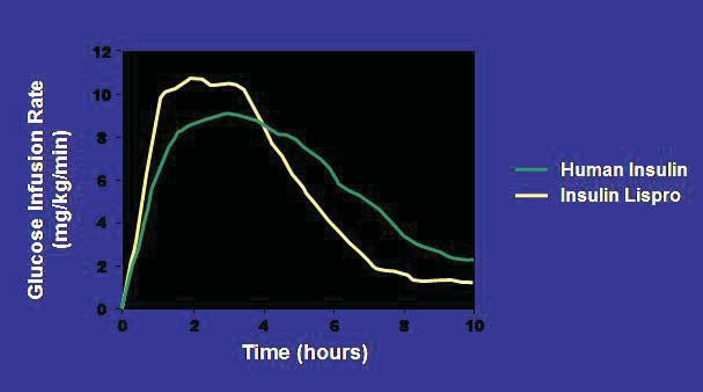
Figure 4a.
Pharmacodynamic Profiles of a Rapid Insulin Analog (insulin lispro) and Regular Insulin (27,28)
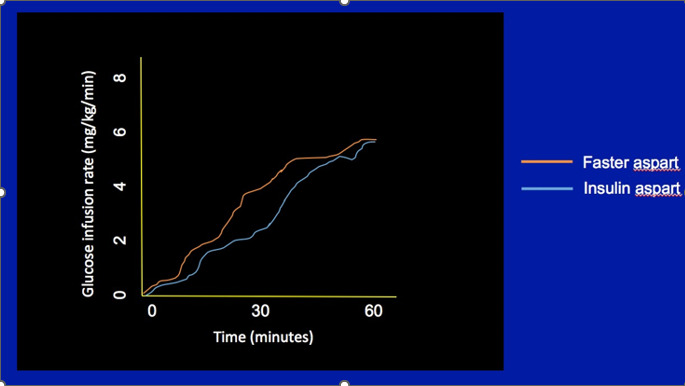
Figure 4b.
Pharmacodynamic Profiles of Faster Aspart and Insulin Aspart (29)

Figure 4c.
Pharmacodynamic Profiles of Long-Acting and Intermediate-Acting Basal Insulins (30,31)
Dose-Dependent Effect
The pharmacodynamics of regular and NPH are particularly affected by the size of the dose (1). Larger doses can cause a delay in the peak and increase the duration of action.
INSULIN PREPARATIONS
Short-Acting (Prandial or Bolus) Regular Insulin
Regular insulin is injected pre-meal to blunt the postprandial rise in glucose levels. It forms hexamers after injection into the SQ space slowing its absorption. Hexameric insulin progressively dissociates into absorbable insulin dimers and monomers. For this reason, regular insulin has a delayed onset of action of 30-60 minutes, and should be injected approximately 30 minutes before the meal to blunt the postprandial rise in blood glucose. Adherence to a 30-minute pre-meal schedule is inconvenient and difficult for many patients.
Rapid-Acting (Prandial or Bolus) Insulin Analogs
Rapid-acting analogs result from changes to the amino acid structure of human insulin which lead to decreases in hexameric insulin formation after injection into the SQ space. This leads to more rapid dissolution of insulin into monomers, more rapid insulin absorption into the bloodstream, and a shorter duration of action. While on a molar basis rapid-acting insulin analogs have identical in vivo potency compared to regular human insulin, higher peak concentrations are achieved (26). For this reason, when converting from regular to a rapid-acting insulin analog, the dose of insulin may need to be reduced. When compared to regular insulin, the rapid-acting insulin analogs lead to less postprandial hyperglycemia and less late postprandial hypoglycemia (32-34). Injection of rapid-acting insulin analogs 15-20 minutes pre-meal leads to maximal reduction of postprandial glucose excursions (35,36), as compared to 30 or more minutes pre-meal for regular insulin. This shorter interval for insulin injection pre-meal is more convenient for patients and leads to greater adherence with prescribed injection timing guidelines. In patients who are unsure of the amount of carbohydrate to be served for a meal, immediate pre-meal dosing allows more accurate dosing and reduces the risk of hypoglycemia. All rapid-acting insulin analogs, except for fast-acting insulin aspart, are approved for use in pumps.
INSULIN LISPRO (HUMALOG)
Insulin lispro (Humalog) results from the reversal of the B28 (proline) and B29 (lysine) amino acid sequence of insulin.
Insulin lispro has been approved for injection before and immediately after a meal. Post-meal insulin dosing is useful for parents of young children with type 1 diabetes, in whom the amount of carbohydrates consumed at a meal can be unpredictable. When compared with pre-meal regular insulin in prepubertal children, post meal insulin lispro showed no significant differences in post meal glucose levels, rates of hypoglycemia, or HbA1c (37). In the rare case of severe human insulin allergy, insulin lispro has been shown to be less immunogenic (38).
INSULIN ASPART (NOVOLOG)
Insulin aspart differs from human insulin by a substitution of the B28 amino acid proline with
aspartic acid. Chemically it is B28-aspartic acid-human insulin. Fast-acting aspart adds 2 excipients, niacinamide and L-arginine, to conventional aspart (39).
INSULIN GLULISINE (APIDRA)
Insulin glulisine differs from human insulin by changes in the amino acid asparagine at position B3 to lysine and the lysine at position B29 to glutamic acid. Chemically, it is 3B-lysine-29B-glutamic acid-human insulin.
INHALED (TECHNOSPHERE) INSULIN (AFREZZA)
Inhaled insulin formulations deliver powdered insulin into the lower airways using an inhaled delivery device. Exubera received FDA approval in 2006 but failed to gain market share and production was discontinued after 1 year. Technosphere insulin (Afrezza) was FDA approved in 2014. Its pulmonary absorption leads to a more rapid absorption than currently available, subcutaneously administered rapid-acting insulin preparations. In subjects with type 2 diabetes, serum insulin levels rise within 5 minutes after inhalation and peak after 17 minutes (40). When compared with pre-meal human regular insulin, technosphere insulin more effectively reduced 4-hour postprandial glucose area under the curve by 52% (41). Only 0.3% of technosphere insulin is detectable in the lungs after 12 hours.
Technosphere insulin leads to a dry cough in 19-30% of subjects tested (40-43). Small reductions in forced expiratory volume (FEV1) are observed in the first 3-6 months of use which are non-progressive for up to 2 years of follow up and reversible after drug discontinuation (42,44,45). The use of technosphere is contraindicated in patients who smoke or have COPD because of alterations in drug absorption. Spirometry needs to be performed prior to initiation of technosphere insulin, after 6 months, and then annually thereafter, with a 20% or higher decline in FEV1 being an indication for drug discontinuation (46).
COMPARISONS OF PRANDIAL INSULINS
No significant differences in glycemic control have been observed in most studies comparing insulin aspart, insulin lispro, and insulin glulisine. Although insulin glulisine exhibits a more rapid onset of action than either insulin lispro or insulin aspart, this does not translate to meaningful clinical differences between these short-acting analog insulins (47).
Faster aspart results in a more rapid onset of action and more glucose lowering within 30 minutes of administration than insulin aspart. However, no significant difference between faster aspart and insulin aspart has been observed in total glucose lowering (48).
Long-Acting (Basal) Insulin Analogs
Long-acting insulins provide basal insulin coverage. Basal insulins suppress hepatic gluconeogenesis to prevent glucose levels from rising during the fasting state in insulin-deficient patients. Among patients with type 1 diabetes, basal insulins additionally prevent ketogenesis.
INSULIN GLARGINE (Lantus)
Insulin glargine (21A-Gly-30Ba-L-Arg-30Bb-L-Arg-human insulin) contains two modifications to human insulin. Two arginines are added to the C-terminus of the B chain shifting the isoelectric point of the insulin from a pH of 5.4 to 6.7 (49). This change makes the insulin more soluble at an acidic pH and insulin glargine is formulated at a pH of 4.0. The second modification is at position A21, where asparagine is replaced by glycine. This substitution prevents deamidation and dimerization that would occur with acid-sensitive asparagine. When insulin glargine is injected into subcutaneous tissue, which is at physiologic pH, the acidic solution is neutralized. Microprecipitates of insulin glargine are formed, from which small amounts of insulin are released throughout a 24-hour period, resulting in a relatively stable level of insulin throughout the day (50). The biological activity of insulin glargine is due to its absorption kinetics and not a different pharmacodynamic activity (e.g., stimulation of peripheral glucose uptake) (51).
Insulin glargine should not be mixed in the same syringe with any another insulin or solution because this will alter its pH and thus affect its absorption profile. Glargine has an onset of action of about 2 hours, and a duration of action of 20-24 hours. It may be given once daily at any time of day, or twice daily at higher doses (typically more than 50 units daily) to better maintain its relatively flat action profile. Its more consistent rate of absorption and lack of a significant peak action result in reduced nocturnal hypoglycemia when insulin glargine is used at bedtime compared with NPH insulin (52,53).
INSULIN DETEMIR (LEVEMIR)
Insulin detemir (Levemir) is a long-acting insulin analog in which the B30 amino acid is omitted and a C14 fatty acid chain (myristic acid) is bound to the B29 lysine amino acid. Insulin detemir is slowly absorbed due to its strong association with albumin in the SQ tissue. When it reaches the bloodstream it again binds to albumin delaying its distribution to the peripheral tissues. Detemir has an onset of action of about 2 hours, and a duration of action of 16-24 hours. It can be given once or twice daily. Patients who experience a rise in glucose levels in the hours prior to a once daily injection due to the waning action of detemir should use a twice daily dosing regimen.
INSULIN DEGLUDEC (TRESIBA)
Insulin degludec (Tresiba) is an ultra-long-acting modified human insulin in which the B30 amino acid is omitted and a glutamic acid spacer links a 16-carbon fatty di-acid chain to the B29 amino acid. Deguldec forms multihexamers following SQ injection, leading to a slow release of insulin monomers into the bloodstream and a prolonged duration of action. The half-life of degludec is about 25 hours and its duration of action more than 42 hours. Flat insulin levels are seen within 3 days of the first injection with less daytime variability when compared with glargine insulin (54). With overall similar HbA1c lowering when compared with glargine insulin, reduced rates of hypoglycemia have been seen with degludec use in type 2 diabetes patients, but not in type 1 diabetes patients (55). No differences in local site reactions, weight gain, or other adverse reactions have been seen with degludec use.
In a preapproval cardiovascular outcomes trial of patients with type 2 diabetes with a history of cardiovascular disease or at high cardiovascular disease risk, insulin degludec was found to be non-inferior to insulin glargine with respect to the likelihood of major adverse cardiovascular events, including cardiovascular death, nonfatal MI, or nonfatal stroke (56). Insulin degludec was associated with less overall symptomatic hypoglycemia in a randomized, controlled trial of patients with type 1 diabetes who were at risk for hypoglycemia, with no significant difference in glycemic control between the two treatment arms (57). Similar results were noted in a randomized, controlled trial of patients with type 2 diabetes on insulin and at risk for hypoglycemia (58).
COMPARISON OF BASAL INSULINS
Compared to NPH, insulin glargine results in significantly less overnight hypoglycemia and a lower rate of hypoglycemic events (59,60). Insulin detemir also results in less overall and nocturnal hypoglycemia compared to NPH (59,61).
Differences have also been noted between U-100 insulin glargine and U-300 insulin glargine. In a study of patients with type 2 diabetes who used mealtime insulin and were on ≥ 42 units insulin daily, U-300 insulin glargine resulted in less nocturnal hypoglycemia compared to U-100 insulin glargine (62). A similar result was seen in a study of patients with type 2 diabetes on basal insulin and oral antihyperglycemic agents (63). In a study of patients with type 2 diabetes who had not previously been treated with insulin, U-300 insulin glargine was associated with a lower risk of hypoglycemia over the study period, although there was no significant difference in the treatment groups in nocturnal hypoglycemia (64). No significant difference in A1C lowering between U-100 glargine and U-300 glargine was noted in these studies (62-64).
Follow-on Biologic Insulins
Relative to the production of other medications, the production of a biologically similar insulin is a more complicated process, which contributes to reduced cost savings in purchasing insulin.(54) Although not termed a biosimilar insulin, Basaglar, a "follow-on biologic" insulin of Lantus or insulin glargine, was approved by the FDA in 2015 (66) Similarly, Admelog is a follow-on insulin of Humalog, or insulin lispro (67).
STORAGE
All insulins have an expiration date on the package labeling which applies to insulins that are unopened and refrigerated.
Unopened insulin (i.e. not previously used) should be stored in the refrigerator at 36°F- 46°F (2°C-8°C). Insulin should never be frozen, kept in direct sunlight, or stored in an ambient temperature greater than 86°F (30°C). Exposure to extremes of temperature can lead to loss of insulin effectiveness and a deterioration in glycemic control. Insulin that has been removal from the original vial (i.e. for pump use) should be used within two weeks or discarded. Insulin vials, cartridges, or pens may be kept at room temperature, between 59°F-86°F (15°C-30°C), for 28 days, or about 1 month. Insulin detemir can be stored at room temperature for up to 42 days.
Regular insulin, the basal insulin analogs (glargine, detemir, and degludec) and the rapid-acting insulin analogs (lispro, aspart and glulisine) are clear and colorless and should not be used if they become cloudy or viscous.
ADVERSE EFFECTS
Hypoglycemia
Hypoglycemia is the most serious adverse effect of insulin therapy and the major barrier to achieving glycemic targets in patients with type 1 diabetes and insulin-requiring type 2 diabetes (68). Intensive insulin therapy in patients with type 1 diabetes in the DCCT was associated with a 2-3 fold increase in severe hypoglycemia (SH), defined as hypoglycemia requiring assistance from others (69). In studies of intensive therapy in type 2 diabetes, including the UKPDS, VADT, ADVANCE, and ACCORD trials, intensive therapy resulted in significantly more common SH when compared with standard therapy (70-73). SH can cause confusion, motor vehicle accidents, seizures and coma, and is estimated to be a cause of death in 4-6% of patients with type 1 diabetes (74,75).
In one study, the adjusted probability of SH was found to range between 1.02 to 3.04% in patients with type 2 diabetes, depending on clinical complexity and intensity of treatment (76). Patients with type 2 diabetes who have had SH are at increased risk of death regardless of the intensity of their glycemic control. Hypoglycemia increases heart rate, systolic blood pressure, myocardial contractility and cardiac output, which may adversely affect those with diabetes who frequently have underlying coronary artery disease (CAD). Glucose levels below 70 mg/dl have been shown to cause ischemic ECG changes in patients with type 2 diabetes and CAD during continuous glucose and ECG monitoring (77). Hypoglycemia may lead to increased mortality due to the pro-arrhythmic effects of sympathoadrenal activation and hypokalemia (78), or from cardiac repolarization, especially in older patients with underlying cardiac disease.
Risk factors for hypoglycemia among insulin-treated patients include older age, longer duration of diabetes, renal insufficiency, hypoglycemia unawareness, prior hypoglycemia, and lower HbA1c (79-82). Avoidance of hypoglycemia therefore takes on particular importance in older patients, given the greater prevalence of cardiovascular disease, cognitive dysfunction, and higher risk of falls and fractures. To help reduce the incidence of hypoglycemia, the American Diabetes Association (ADA) advises targeting a higher HbA1c of less than 8% in patients who are older, with a longer duration of disease, more comorbidities, frequent hypoglycemia and underlying cardiovascular disease (83).
All patients receiving insulin should learn to recognize the symptoms of hypoglycemia and how best to treat low glucose levels.
Weight Gain
Weight gain is a common side effect of insulin therapy. In part, the weight gain can be a result of frequent hypoglycemic episodes in which patients consume extra calories to treat the low glucose level and often overeat in response to hunger. One of the anabolic effects of insulin is to promote the uptake of fatty acids into adipose tissue. The amount of weight gain in the DCCT (type 1 patients) and UKPDS (type 2 patients) associated with insulin therapy was 4.6 kg and 4.0 kg respectively (69,70). Less weight gain is encountered with detemir insulin than with NPH or glargine insulin (84,85). The etiology of lower weight gain with detemir when compared with NPH or glargine is not entirely understood (86). Basal insulin added to oral antihyperglycemic agents leads to less weight gain than either biphasic insulin aspart or prandial aspart insulin (65). Lispro mix 75/25 insulin leads to greater weight gain than glargine insulin when added to oral antihyperglycemic agents (87).
Local Reactions
True allergic reactions and cutaneous reactions are rare with human insulin and insulin analogs. Hypersensitivity reactions can rarely develop in response to the insulin or one of its additives (protamine for example) and can result in local erythema, pruritus, a wheal or more systemic reactions including anaphylaxis. Successful approaches to insulin allergies include continuous subcutaneous insulin infusions, and use of lispro insulin which appears to be less allergenic (38,88).
Lipoatrophy was common with use of less pure and animal insulins, but is no longer encountered. To avoid the lipohypertrophic effects of insulin, patients should be instructed to rotate their insulin injection sites, preferably rotating within one area and not reusing for one week
Mitogenic Properties
Several retrospective, observational studies have shown correlations between insulin dose and cancer risk for most insulin types (human insulin, aspart, lispro or glargine) (89-91). These observational studies assessed large patient databases and have significant, inherent limitations, such as the potential for different pre-treatment characteristics of the groups, selection bias, the small numbers of cancer cases found, and short duration of follow-up. Meta-analyses of studies comparing exogenous insulin to non-insulin antihyperglycemic therapies have shown associations of insulin with several cancers (14,15). However, there are also inherent limitations to such analyses. In a randomized, 5-year, open-label trial comparing the progression of retinopathy in NPH and insulin glargine users, no increased risk of cancer was found in the 1,017 patient sample (92). In an analysis of 31 randomized controlled trials from the Sanofi-Aventis safety database (phase 2, 3, and 4 studies), insulin glargine was not associated with an increased risk of cancer (93). The 7-year, randomized ORIGIN trial assessed the cardiovascular effects of insulin glargine versus standard care in more than 12,500 individuals with diabetes or pre-diabetes and found no increased risk of all-cancer-combined or of cancer mortality among glargine-treated individuals (94). A recent review of large epidemiologic studies did not find evidence of an increased risk of malignancy among glargine-treated patients when compared with other insulin therapies (15).
Cardiovascular Disease
Among intensively controlled patients in the VADT (Veterans Affairs Diabetes Trial), ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation), and ACCORD (Action to Control Cardiovascular Risk in Diabetes), a higher proportion (41–90%) required insulin therapy than among the standard control groups (24–74%) (71-73). Nonsignificant reductions in cardiovascular events were seen with intensive diabetes control when compared with standard control in ADVANCE, ACCORD, and VADT respectively. An increased mortality rate was observed in ACCORD after 3.5 years of intensive therapy when patients were targeted to an HbA1c of less than 6.0%, 73% of whom received insulin. However, mortality was not temporally associated with severe hypoglycemia. The results of ACCORD support less aggressive diabetes management among patients at high risk for a cardiovascular event. The 7-year, randomized ORIGIN trial assessed the cardiovascular effects of insulin glargine versus standard care in more than 12,500 individuals with diabetes or pre-diabetes and found no increased risk of cardiovascular events or of cardiovascular mortality among glargine-treated individuals (94).
TYPES OF REGIMENS
General Principles
TYPE 1 DIABETES
Autoimmune beta cell destruction results in a progressive decline in insulin production in patients with type 1 diabetes who eventually require insulin for survival. Patients with type 1 diabetes generally require a replacement dose of 0.5-1.0 units per kg of body weight per day of insulin (95). During the early stages of type 1 diabetes, patients commonly require less insulin because remaining beta cells still produce some insulin; during their "honeymoon period" insulin requirements can be in the range of 0.2-0.6 units per kg per day (95,96). Intensive insulin therapy (defined as 3 or more insulin injections daily or insulin pump therapy) is indicated for patients with type 1 diabetes to provide better glycemic control with less glucose variability than 1 or 2 daily injections, and reduce the development and progression of microvascular and macrovascular complications (69,97,98).
TYPE 2 DIABETES
The slowly progressive beta cell loss in patients with type 2 diabetes means many patients with type 2 diabetes will eventually require insulin therapy to attain adequate glycemic control. Initiation of basal insulin can be considered in any of the following situations: 1) a patient with an HbA1C > 11 with concern for insulin deficiency; 2) a patient without atherosclerotic cardiovascular disease and/or chronic kidney disease with an HbA1C above goal after 3 months of metformin monotherapy; 3) a patient with atherosclerotic cardiovascular disease and/or chronic kidney disease with an HbA1C above goal after 3 months of treatment with metformin, a GLP-1 receptor agonist, and/or an SGLT2 inhibitor (99). Since type 2 diabetes is associated with insulin resistance, insulin requirements can exceed 1 unit/kg/day. When initiating insulin therapy in patients with type 2 diabetes, basal insulin is often used in combination with other non-insulin antihyperglycemic medications a patient is taking. An intermediate or long-acting insulin (e.g., NPH, insulin glargine, or insulin detemir) is added at bedtime, and the dose titrated to attain a target fasting glucose (100) .
Basal insulin is effective at lowering HbA1c when added to oral hypoglycemic agents starting at a dose of 10 U daily or 0.2 U/kg. When used in patients uncontrolled on oral agents, basal insulin lowers HbA1c 1.2–1.5% (65,85). In these treat-to-target studies, patients were instructed to titrate their basal insulin dosages up every 2–3 days by 1–4 units based on algorithms to achieve fasting plasma glucose (FPG) levels in the 70- to 126-mg/dl range. Those studies targeting a FPG < 108 mg/dl achieve modestly better success in achieving an HbA1c < 7% (63.2 vs. 52%) than those targeting a FPG of less than 126 mg/dl, with mildly higher rates of hypoglycemia (65,85).
Basal insulin, by suppressing hepatic glucose output during the night, will control the fasting blood glucose (FPG), while the other antihyperglycemic medications continue to control postprandial glucose levels throughout the day (101). A starting dose of 10 units of basal insulin is commonly utilized, though starting a dose of 0.1-0.2 units/kg will more rapidly attain the target fasting glucose level (102). In patients whose fasting glucose levels become well controlled with basal insulin, but whose glucose levels rise significantly high later in the day with a persistently elevated HbA1C, prandial insulin is indicated. At this point, the patient is experiencing beta-cell failure. If the patient is taking an insulin secretagogue (e.g., a sulfonylurea or meglitinide) it should be discontinued, as insulin will now be replaced exogenously. However, other agents not having a predominantly insulin-stimulating effect should be continued.
GOALS OF THERAPY
Before starting a patient on insulin, or adjusting their current insulin therapy, it is important to establish glycemic goals tailored to the patient. The American Diabetes Association currently recommends individualized glycemic goals (103). Those with a longer duration of diabetes, shorter life expectancy, presence of important comorbidities or established vascular complications, and at higher risk of hypoglycemia should have higher glycemic targets, with an A1C of < 8% reasonable for those with the least to gain from more intensive control and at highest risk for adverse outcomes from hypoglycemia. For the majority of patients who are otherwise healthy, glycemic targets include the following: preprandial plasma glucose 80-130 mg/dl; postprandial plasma glucose <180 mg/dl; and A1C <7% (103).
In the DCCT, retinopathy initially worsened during the first year in patients with type 1 diabetes who received intensive therapy (69). This was associated with rapid lowering of glucose levels. Thus, in patients with proliferative retinopathy or those with underlying non-proliferative diabetic retinopathy and a high A1C (e.g., >10%), slower lowering of glucose is warranted. Another example of individualizing glycemic goals is a patient with hypoglycemic unawareness; glycemic goals should be less aggressive as glucose levels should not approach 80 mg/dl too closely (98).
REPLACEMENT STRATEGIES
Physiologic Insulin Replacement
A functioning pancreas releases insulin continuously, to supply a basal amount to suppress hepatic glucose output and prevent ketogenesis between meals and overnight, and also releases a bolus of insulin prandially to promote glucose utilization after eating.(90) Replacing insulin in a manner that attempts to mimic physiologic insulin release is commonly referred to as basal/bolus insulin therapy. Physiologic replacement requires multiple daily injections (3 or more) or use of an insulin pump. Basal insulin requirements are approximately 50% of the total daily amount. Prandial insulin is 50-60% of the total daily insulin requirement administered before meals (96). Providing basal-bolus insulin regimens allows patients to have flexibility in their mealtimes and achieve better glycemic control.
Non-Physiologic Insulin Replacement
When insulin is given once or twice daily, insulin levels do not mimic physiologic insulin release patterns. For people with type 2 diabetes, in whom bolus insulin replacement is not as critical, once or twice daily basal insulin injection regimens often work well with reasonable glycemic control achieved.
In patients with type 2 diabetes, a starting daily basal insulin dose can be calculated by multiplying 0.1 or 0.2 by the patient's weight in kilograms and increased after taking into account factors such as hyperglycemia (99). The basal insulin dose in type 2 patients is adjusted to attain a target fasting glucose level. The patient's other non-insulin anti-hyperglycemic agents then can better control daytime glucose levels.
The current American Diabetes Association guidelines recommend that if a patient's A1C is not at goal despite the use of basal insulin attaining target fasting glucose levels, then an additional injection of prandial insulin, with a starting dose comprised of 10% of the daily basal insulin dose, can be added before the most sizable meal of the day. Prandial insulin can be titrated based on blood glucose measurements by 10-15% twice a week. If glycemic control is suboptimal, then more prandial insulin injections can be added before other meals (99).
EXAMPLES OF REGIMENS
Once Daily Insulin Regimen (for patients with type 2 diabetes on oral agents)
NPH (Figure 5a), insulin glargine (Figure 5b), or insulin detemir are most often given at bedtime (however insulin glargine and insulin degludec can be administered anytime of the day) (104) ; or for patients who eat large amounts of carbohydrates at dinner, an insulin mixture, regular and NPH or a premixed insulin, can be given prior to dinner (Figure 5c).
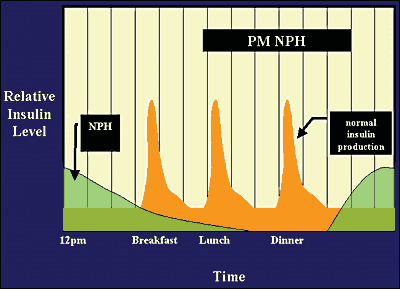
Figure 5a.
PM NPH Administration
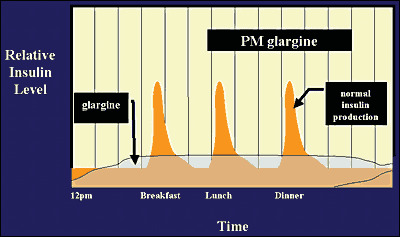
Figure 5b.
Glargine Administration

Figure 5c.
NPH and Regular Insulin at Dinner
Twice-Daily Insulin Regimen (Split-Mixed and Pre-Mixed Regimens)
Two-thirds of the insulin dose is typically given in the morning before breakfast and one-third is given before dinner. Premixed insulins can be used or a mixture of a short-acting insulin (e.g., regular, insulin aspart/glulisine/lispro) and an intermediate-acting insulin (e.g., NPH) (Figure 6a) (96).
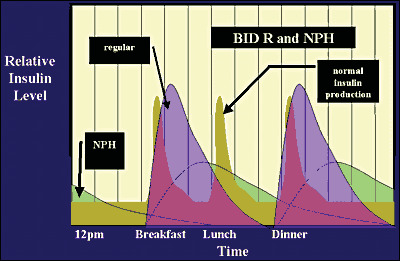
Figure 6a.
NPH and Twice a Day Regular Insulin
2/3 total daily dose at breakfast: given as 2/3 NPH and 1/3 Regular (or insulin aspart/glulisine/lispro)
1/3 total daily dose at dinner: divided in equal amounts of NPH and Regular (or insulin aspart/glulisine/lispro)
For patients who experience nocturnal hypoglycemia when NPH is administered at dinner with a short-acting insulin, moving the NPH dose to bedtime helps reduce the risk for nocturnal hypoglycemia (105). Conversely, NPH at dinner can result in fasting hyperglycemia due to dissipation of insulin activity and the early morning rise in counter-regulatory hormones cortisol and growth hormone (the dawn phenomenon). Moving the NPH dose to bedtime can also help resolve this problem (106) (Figure 6b). An obvious limitation to using premixed insulin is reduced flexibility in dosing; if the dose is adjusted, both types of insulin in the mixture will be adjusted.

Figure 6b.
Twice a Day NPH and Regular
Multiple Daily Insulin Injection Regimen: Basal plus Prandial Insulin
Many different types of regimens are possible with multiple daily injections. Regular, insulin aspart, glulisine and lispro are used to provide prandial insulin. NPH, insulin glargine, insulin detemir, and insulin degludec are used to provide basal insulin.
Regular, insulin aspart/glulisine/lispro before meals and NPH, insulin glargine, insulin detemir, or insulin degludec at bedtime (hs) (Figure 7a, 7b).
Insulin aspart/glulisine/lispro before meals and NPH twice daily (breakfast and bedtime) (Figure 8).

Figure 7a.
Bedtime NPH and Regular Insulin with Meals

Figure 7b.
Bedtime Glargine Insulin and Lispro/Aspart with Meals
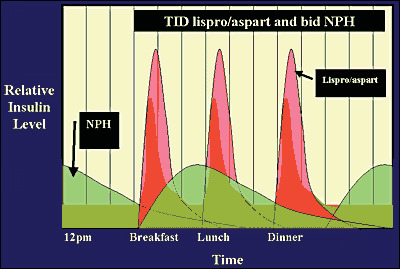
Figure 8.
NPH Twice a Day and Lispro/Aspart with Meals
Insulin Pump Therapy
Insulin pump or continuous subcutaneous insulin infusion (CSII) therapy is another option for intensive insulin therapy using only rapid-acting insulin. Insulin pump therapy is indicated in patients with type 1 diabetes, and in those with markedly insulin-deficient type 2 diabetes (107). Patients initiated on insulin pump therapy need to have been trained in the components of intensive diabetes management or will not gain significant benefit from conversion to insulin pump therapy. The components of intensive diabetes management include knowledge of carbohydrate counting and adjustments in the insulin bolus dose based on the carbohydrate content of meals and snacks, the measured glucose level, and the amount and duration of exercise. Some insulin pumps are able to deliver insulin boluses in as low as 0.01-unit increments, ideal for patients who are insulin sensitive. The basal insulin infusion can be delivered in as low as 0.001-unit increments and can be adjusted based on an individual patient's needs. Basal rate requirements are typically higher in the early morning hours to counter the dawn rise in glucose levels and lower in the afternoon when patients are more active and overnight when patients are at rest. Temporary basal rates can be programmed to be increased during times of inactivity or illness when insulin requirements are higher, and decreased when physically active and insulin requirements are reduced.
The bolus calculator function of insulin pumps helps patients determine insulin bolus doses required for the carbohydrate content of foods and the measured glucose level. After a patient enters this information into the pump, a recommended bolus dose is displayed by the pump based on the patient's insulin-to-carb ratio and insulin sensitivity factor. This function is especially helpful when a patient needs to determine the amount of supplemental insulin required to correct a high postprandial glucose level. The pump takes into account the active insulin remaining from the pre-meal bolus (insulin-on-board), and recommends a reduced corrective supplemental insulin dose, thereby preventing insulin stacking and hypoglycemia.
Potential benefits of insulin pumps include less weight gain, less hypoglycemia, and lowering of hemoglobin A1c levels when compared to multiple daily injections (108-111). The addition of continuous glucose monitoring to patients on insulin pumps has been shown to further improve glycemic control and reduce the frequency of symptomatic and severe hypoglycemia. Insulin pumps are available with a threshold suspend function which can discontinue the basal insulin infusion for up to a period of 2.5 hours when the monitor detects a low glucose level that is untreated. This prevents a further decline in glucose levels. To date, one hybrid closed loop system exists that has an "Auto Mode," in which the basal rate of the insulin pump is adjusted up or down every 5 minutes based on data from the continuous glucose monitoring (CGM) system to achieve a target glucose of 120 mg/dl (112).
Timing of Prandial Insulin Injections
The onset of action of regular insulin is approximately 30 minutes; while insulin aspart/glulisine/lispro can be detected systemically within 15 minutes after a subcutaneous bolus is given. The timing of the pre-meal insulin bolus can be reduced when the measured glucose level is low and lengthened when hyperglycemia is present before eating. To best match the insulin action with the glycemic effect of meals, regular insulin is optimally given 30 minutes before the meal and the rapid-acting insulins 15-20 minutes before the meal. Insulin pumps and multi-dose insulin injection regimens using basal analog insulin combined with a rapid-acting insulins provide patients with the greatest flexibility of varying the time of meals without sacrificing an increased risk of hypoglycemia, when compared with NPH-based insulin regimens.
ADJUSTMENTS
Insulin doses should be adjusted to achieve glycemic targets. Typically, a 10-20% increase or decrease in an insulin dose is appropriate, based on the degree of hyper- or hypoglycemia, and the insulin sensitivity of the patient. Hypoglycemia that is frequent or severe should prompt an immediate reduction in the responsible insulin dose. Increases to insulin doses should be based on the occurrence of consistently high glucose levels at a particular time of day, rather than periodic glucose elevations that are more likely diet-mediated.
Adjustment of Intermediate to Long-Acting Insulin
When a dose of intermediate or long-acting insulin is adjusted, it is recommended to wait at least 3-5 days before further changes in the dose to assess the response (96).
Adjustment of Once-Daily Evening Insulin
Basal insulin can be started either using 10 units or 0.1-0.2 units/kg body weight at bedtime. The FPG is used to adjust the intermediate (NPH), long-acting insulin (glargine, detemir, or degludec) given in the evening. Algorithms provided to patients to adjust their basal insulin dose based on fasting glucose levels have been shown to improve glycemic control (113). The algorithm should target the fasting glucose range of 80-130 mg/dl (103). An example of a forced titration schedule is show below (Table 4):
Table 4.
Forced Titration Algorithm
View in own window
| Fasting Glucose the past 3 Days | Increase in Basal Insulin (units) |
|---|---|
| 80-130 | 0 |
| 130-159 | 2 |
| 160-189 | 4 |
| 190-220 | 6 |
| Over 220 | 8 |
| Decrease dose by 2-4 units for any glucose level < 80 | |
Lower dose adjustments are used for more insulin sensitive patients (usually type 1 patients) and higher doses for more insulin resistant patients (usually those with type 2 diabetes). A simple algorithm for patients with type 2 diabetes recommends adjusting the basal insulin dose by 2 units every 2 to 3 days if fasting glucose levels are consistently above the target upper range (103) .
Carbohydrate Counting
In patients on set dose of prandial insulin, post meal glucose variability can be controlled by having patients keep the carbohydrate content of the meal similar at mealtimes from day to day. A more sophisticated type of prandial insulin regimen is one in which a patient doses their prandial insulin based on the number of carbohydrates eaten at the meal. By learning how to count carbohydrates, and dosing their insulin accordingly, patients are afforded flexibility in the carbohydrate content of their meals. The rule of 500 can be used to approximate the amount of carbohydrates covered by 1 unit of prandial insulin, termed the insulin to carbohydrate ratio (ICR), using the total daily dose (TDD) of insulin:
Calculation of the insulin to carbohydrate ratio:
ICR= 500/TDD
For example, for a patient using 60 units of insulin per day, the ICR would be 500/60 or approximately 1:8, or 1 unit for each 8 grams of carbohydrate in the meal or snack.
This ratio is adjusted based on post meal glucose levels and may be different for each meal. The ICR is adjusted to attain post meal glucose levels in the target range (usually 100-180 mg/dl). The ICR can also be used for snacks (115). Carbohydrate counting can be challenging for some patients. Education in medical nutrition therapy is critical for patients on insulin.
A comprehensive diabetes education class that teaches self-management skills, such as how to dose prandial insulin by matching it to the amount of carbohydrate intake is an excellent resource to facilitate patients in adopting an intensive insulin therapy regimen (116).
Adjustments for Exercise
Exercise improves insulin sensitivity. Thus, when a patient exercises, it is often necessary to decrease the insulin dose (and/or increase caloric intake) to prevent hypoglycemia. For morning exercise, the pre-breakfast insulin dose should be reduced (by about 25%) depending on the duration and intensity of the exercise. For late-morning/early-afternoon and evening exercise, the pre-lunch and pre-dinner insulin dose should be reduced respectively (117). The effect of exercise on insulin sensitivity can last for many hours; so more than 1 insulin dose may need to be adjusted. After more prolonged exercise, the bedtime long acting insulin dose may need to be reduced should there be a pronounced fall in overnight glucose levels.
SELF-MONITORING OF BLOOD GLUCOSE
Self-monitoring of blood glucose (SMBG) allows patients and physicians to recognize glucose trends to guide insulin dosage adjustments. In those using short or rapid-acting inulin, SMBG also provides a patient with the information needed to give an accurate supplemental insulin dose to return a high glucose level back to the target glucose range. Studies in patients with type 1 diabetes have shown a progressive reduction in hemoglobin A1C levels with more frequent glucose monitoring.(118) Currently, the ADA recommends that patients with diabetes on multiple daily injections of insulin or on an insulin pump check blood glucose before eating, exercise, and bedtime, with symptoms of hypoglycemia, and sometimes after meals. For patients with type 2 diabetes not on multiple daily injections of insulin, no specific frequency of SMBG is recommended but rather it is recommended that SMBG and its assessment be a part of patients' treatment and management plan (118). Most glucose meters are now plasma-referenced, correlating better to the ADA's glycemic goals. Plasma glucose concentrations are approximately 10-15% higher than whole blood glucose concentrations (119).
CGM, which measures interstitial glucose, is available in 2 forms: an intermittent or "flash" CGM system and a real-time CGM system (120). To date, the intermittent CGM system and one real-time CGM system do not require calibration with blood glucose. Intermittent CGM has been associated with less time spent in hypoglycemia in patients with type 1 diabetes and in patients with type 2 diabetes (121,122), and the real-time CGM has been associated with improved glycemic control, more so when used consistently, and less time spent in hypoglycemia, and less severe hypoglycemia in patients with type 1 diabetes.(123,124)
SICK DAY GUIDELINES
A common misconception among patients is that if they are sick enough that they don't eat or vomit, they should hold off on taking their anti-hyperglycemic medications, insulin included. Patients who are ill should be instructed to continue their basal insulin therapy, maintain fluid intake, eat smaller meals as tolerated, and test their glucose levels every 1-4 hours (ketones as well for people with type 1 diabetes when glucose levels are over 200 mg/dl). Supplemental insulin doses to correct hyperglycemia can be given up to every 4 hours as needed for persistent hyperglycemia, or more often when the insulin on board from is taken into account. For patients using the bolus calculator function of their insulin pump, the recommend bolus dose to correct an elevated glucose level automatically takes into account the insulin still active (insulin on board) from prior insulin boluses. If the glucose is >240 mg/dl with large ketonuria, patients should contact their provider immediately, or proceed to an emergency room for treatment of ketoacidosis using intravenous fluids and insulin (85).
ACKNOWLEDGEMENTS
The prior version of this chapter was extensively modified based on a previous chapter written by Lisa Kroon, PharmD, CDE, Ira D. Goldfine, M.D. and Sinan Tanyolac, M.D.
REFERENCES
- 1.
-
Binder CB, J. In: Porte D, Jr.; Sherwin, R, ed. Elenberg's and Rifkin's Diabetes Mellitus. 5th edition ed. Stamford, CT: Appleton and Lange; 1996:689.
- 2.
- 3.
-
Humalog [package insert]. Eli Lilly and Company, Indianapolis, IN. 2018.
- 4.
-
Humalog Mix75/25 [package insert]. Eli Lilly and Company, Indianapolis, IN. 2018.
- 5.
-
Apidra [package insert]. Sanofi, Bridgewater, NJ. 2015.
- 6.
-
Levemir [package insert]. Novo Nordisk, Plainsboro, NJ. 2015.
- 7.
-
Lantus [package insert]. Sanofi, Bridgewater, NJ. 2015.
- 8.
-
Novolog [package insert]. Novo Nordisk, Plainsboro, NJ. 2018.
- 9.
-
Novolog Mix 70/30 [package insert]. Novo Nordisk, Plainsboro, NJ. 2018.
- 10.
-
Humalog Mix50/50 [package insert]. Eli Lilly and Company, Indianapolis, IN. 2018.
- 11.
-
Tresiba [package insert]. Novo Nordisk, Plainsboro, NJ. 2018.
- 12.
-
Kurtzhals P, Schaffer L, Sorensen A, Kristensen C, Jonassen I, Schmid C, et al. Correlations of receptor binding and metabolic and mitogenic potencies of insulin analogs designed for clinical use. Diabetes. 2000;49:999–1005. [PubMed: 10866053]
- 13.
-
Mussig K, Staiger H, Kantartzis K, Fritsche A, Kanz L, Haring HU. Type 2 diabetes mellitus and risk of malignancy: is there a strategy to identify a subphenotype of patients with increased susceptibility to endogenous and exogenous hyperinsulinism? Diabet Med. 2011;28:276–86. [PubMed: 21309835]
- 14.
-
Karlstad O, Starup-Linde J, Vestergaard P, Hjellvik V, Bazelier MT, Schmidt MK, et al. Use of insulin and insulin analogs and risk of cancer - systematic review and meta-analysis of observational studies. Curr Drug Saf. 2013;8:333–48. [PMC free article: PMC3899599] [PubMed: 24215311]
- 15.
-
Janghorbani M, Dehghani M, Salehi-Marzijarani M. Systematic review and meta-analysis of insulin therapy and risk of cancer. Horm Cancer. 2012;3:137–46. [PubMed: 22528451]
- 16.
-
Nishimura E, Sorensen AR, Hansen BF, Stidsen CE, Olsen GS, Schaffer L, Bonnesen C, Hegelund AC, Lundby A, Jonassen I. Insulin Degludec Is a New Generation Ultra-Long Acting Basal Insulin Designed To Maintain Full Metabolic Effect While Minimizing Mitogenic Potential. Diabetologia. 2010;53:S388.
- 17.
-
Schernthaner G. Immunogenicity and allergenic potential of animal and human insulins. Diabetes Care. 1993;16 Suppl 3:155–65. [PubMed: 8299472]
- 18.
-
Vardar B, Kizilci S. Incidence of lipohypertrophy in diabetic patients and a study of influencing factors. Diabetes Res Clin Pract. 2007;77:231–6. [PubMed: 17303282]
- 19.
-
Pearson SM, Trujillo JM. Conversion from insulin glargine U-100 to insulin glargine U-300 or insulin degludec and the impact on dosage requirements. Ther Adv Endocrinol Metab. 2018;9:113–21. [PMC free article: PMC5871063] [PubMed: 29619208]
- 20.
-
Kroon LA, Assemi M, Carlisle BA. Diabetes Mellitus. In: Koda-Kimble MA, Young LY, Alldredge BA, Corelli RL, Guglielmo BJ, Kradjan WA, Williams BR., ed. Applied Therapeutics: The Clinical Use of Drugs, 9th Edition. Baltimore, MD: Lippincott, Williams and Wilkins; 2009.
- 21.
-
ter Braak EW, Woodworth JR, Bianchi R, Cerimele B, Erkelens DW, Thijssen JH, et al. Injection site effects on the pharmacokinetics and glucodynamics of insulin lispro and regular insulin. Diabetes Care. 1996;19:1437–40. [PubMed: 8941480]
- 22.
-
Nosek L, Coester HV, Roepstorff C, Thomsen HF, Kristensen NR, Haahr H, et al. Glucose-lowering effect of insulin degludec is independent of subcutaneous injection region. Clin Drug Investig. 2014;34:673–9. [PMC free article: PMC4143594] [PubMed: 25124362]
- 23.
-
Home PD, Ashwell SG. An overview of insulin glargine. Diabetes Metab Res Rev. 2002;18 Suppl 3:S57–63. [PubMed: 12324987]
- 24.
-
Duckworth WC, Bennett RG, Hamel FG. Insulin degradation: progress and potential. Endocr Rev. 1998;19:608–24. [PubMed: 9793760]
- 25.
-
MS N, Karam J. Pancreatic Hormones and Antidiabetic Drugs. In: B; K, ed. Basic and Clinical Pharmacology, 8th Edition. New York: Lange Medical Books/McGraw Hill; 2001:711-34.
- 26.
-
Rabkin R, Ryan MP, Duckworth WC. The renal metabolism of insulin. Diabetologia. 1984;27:351–7. [PubMed: 6389240]
- 27.
-
Roach P, Woodworth JR. Clinical pharmacokinetics and pharmacodynamics of insulin lispro mixtures. Clin Pharmacokinet. 2002;41:1043–57. [PubMed: 12403642]
- 28.
-
Rave K, Bott S, Heinemann L, Sha S, Becker RH, Willavize SA, et al. Time-action profile of inhaled insulin in comparison with subcutaneously injected insulin lispro and regular human insulin. Diabetes Care. 2005;28:1077–82. [PubMed: 15855570]
- 29.
-
Biester T, Kordonouri O, Danne T. Pharmacological Properties of Faster-Acting Insulin Aspart. Curr Diab Rep. 2017;17:101. [PubMed: 28940145]
- 30.
-
Plank J, Bodenlenz M, Sinner F, Magnes C, Gorzer E, Regittnig W, et al. A double-blind, randomized, dose-response study investigating the pharmacodynamic and pharmacokinetic properties of the long-acting insulin analog detemir. Diabetes Care. 2005;28:1107–12. [PubMed: 15855574]
- 31.
-
Lepore M, Pampanelli S, Fanelli C, Porcellati F, Bartocci L, Di Vincenzo A, et al. Pharmacokinetics and pharmacodynamics of subcutaneous injection of long-acting human insulin analog glargine, NPH insulin, and ultralente human insulin and continuous subcutaneous infusion of insulin lispro. Diabetes. 2000;49:2142–8. [PubMed: 11118018]
- 32.
-
Pampanelli S, Torlone E, Ialli C, Del Sindaco P, Ciofetta M, Lepore M, et al. Improved postprandial metabolic control after subcutaneous injection of a short-acting insulin analog in IDDM of short duration with residual pancreatic beta-cell function. Diabetes Care. 1995;18:1452–9. [PubMed: 8722069]
- 33.
-
Brunelle BL, Llewelyn J, Anderson JH Jr, Gale EA, Koivisto VA. Meta-analysis of the effect of insulin lispro on severe hypoglycemia in patients with type 1 diabetes. Diabetes Care. 1998;21:1726–31. [PubMed: 9773738]
- 34.
-
Lalli C, Ciofetta M, Del Sindaco P, Torlone E, Pampanelli S, Compagnucci P, et al. Long-term intensive treatment of type 1 diabetes with the short-acting insulin analog lispro in variable combination with NPH insulin at mealtime. Diabetes Care. 1999;22:468–77. [PubMed: 10097931]
- 35.
-
Cobry E, McFann K, Messer L, Gage V, VanderWel B, Horton L, et al. Timing of meal insulin boluses to achieve optimal postprandial glycemic control in patients with type 1 diabetes. Diabetes Technol Ther. 2010;12:173–7. [PubMed: 20151766]
- 36.
-
Luijf YM, van Bon AC, Hoekstra JB, Devries JH. Premeal injection of rapid-acting insulin reduces postprandial glycemic excursions in type 1 diabetes. Diabetes Care. 2010;33:2152–5. [PMC free article: PMC2945151] [PubMed: 20693354]
- 37.
-
Tupola S, Komulainen J, Jaaskelainen J, Sipila I. Post-prandial insulin lispro vs. human regular insulin in prepubertal children with Type 1 diabetes mellitus. Diabet Med. 2001;18:654–8. [PubMed: 11553203]
- 38.
-
Kumar D. Lispro analog for treatment of generalized allergy to human insulin. Diabetes Care. 1997;20:1357–9. [PubMed: 9283778]
- 39.
-
Heise T, Hovelmann U, Zijlstra E, Stender-Petersen K, Jacobsen JB, Haahr H. A Comparison of Pharmacokinetic and Pharmacodynamic Properties Between Faster-Acting Insulin Aspart and Insulin Aspart in Elderly Subjects with Type 1 Diabetes Mellitus. Drugs Aging. 2017;34:29–38. [PMC free article: PMC5222895] [PubMed: 27873152]
- 40.
-
Rave K, Heise T, Heinemann L, Boss AH. Inhaled Technosphere insulin in comparison to subcutaneous regular human insulin: time action profile and variability in subjects with type 2 diabetes. J Diabetes Sci Technol. 2008;2:205–12. [PMC free article: PMC2771503] [PubMed: 19885344]
- 41.
-
Rave K, Heise T, Pfutzner A, Boss AH. Coverage of postprandial blood glucose excursions with inhaled technosphere insulin in comparison to subcutaneously injected regular human insulin in subjects with type 2 diabetes. Diabetes Care. 2007;30:2307–8. [PubMed: 17586744]
- 42.
-
Rosenstock J, Bergenstal R, Defronzo RA, Hirsch IB, Klonoff D, Boss AH, et al. Efficacy and safety of Technosphere inhaled insulin compared with Technosphere powder placebo in insulin-naive type 2 diabetes suboptimally controlled with oral agents. Diabetes Care. 2008;31:2177–82. [PMC free article: PMC2571070] [PubMed: 18678610]
- 43.
-
Rosenstock J, Lorber DL, Gnudi L, Howard CP, Bilheimer DW, Chang PC, et al. Prandial inhaled insulin plus basal insulin glargine versus twice daily biaspart insulin for type 2 diabetes: a multicentre randomised trial. Lancet. 2010;375:2244–53. [PubMed: 20609970]
- 44.
-
Raskin P, Heller S, Honka M, Chang PC, Boss AH, Richardson PC, et al. Pulmonary function over 2 years in diabetic patients treated with prandial inhaled Technosphere Insulin or usual antidiabetes treatment: a randomized trial. Diabetes Obes Metab. 2012;14:163–73. [PubMed: 21951325]
- 45.
-
Rosenstock J, Cefalu WT, Hollander PA, Klioze SS, Reis J, Duggan WT. Safety and efficacy of inhaled human insulin (exubera) during discontinuation and readministration of therapy in adults with type 2 diabetes: a 3-year randomized controlled trial. Diabetes Technol Ther. 2009;11:697–705. [PubMed: 19905885]
- 46.
-
Afrezza [package insert]. MannKind Corporation, Danbury, CT. 2018.
- 47.
-
Home PD. The pharmacokinetics and pharmacodynamics of rapid-acting insulin analogues and their clinical consequences. Diabetes Obes Metab. 2012;14:780–8. [PubMed: 22321739]
- 48.
-
Heise T, Stender-Petersen K, Hovelmann U, Jacobsen JB, Nosek L, Zijlstra E, et al. Pharmacokinetic and Pharmacodynamic Properties of Faster-Acting Insulin Aspart versus Insulin Aspart Across a Clinically Relevant Dose Range in Subjects with Type 1 Diabetes Mellitus. Clin Pharmacokinet. 2017;56:649–60. [PMC free article: PMC5425492] [PubMed: 27878566]
- 49.
-
Bolli GB, Owens DR. Insulin glargine. Lancet. 2000;356:443–5. [PubMed: 10981882]
- 50.
-
Heinemann L, Linkeschova R, Rave K, Hompesch B, Sedlak M, Heise T. Time-action profile of the long-acting insulin analog insulin glargine (HOE901) in comparison with those of NPH insulin and placebo. Diabetes Care. 2000;23:644–9. [PubMed: 10834424]
- 51.
-
Mudaliar S, Mohideen P, Deutsch R, Ciaraldi TP, Armstrong D, Kim B, et al. Intravenous glargine and regular insulin have similar effects on endogenous glucose output and peripheral activation/deactivation kinetic profiles. Diabetes Care. 2002;25:1597–602. [PubMed: 12196433]
- 52.
-
Yki-Jarvinen H, Dressler A, Ziemen M. Group HOEsS. Less nocturnal hypoglycemia and better post-dinner glucose control with bedtime insulin glargine compared with bedtime NPH insulin during insulin combination therapy in type 2 diabetes. HOE 901/3002 Study Group. Diabetes Care. 2000;23:1130–6. [PubMed: 10937510]
- 53.
-
Ratner RE, Hirsch IB, Neifing JL, Garg SK, Mecca TE, Wilson CA. Less hypoglycemia with insulin glargine in intensive insulin therapy for type 1 diabetes. U.S. Study Group of Insulin Glargine in Type 1 Diabetes. Diabetes Care. 2000;23:639–43. [PubMed: 10834423]
- 54.
-
Heise T, Hermanski L, Nosek L, Feldman A, Rasmussen S, Haahr H. Insulin degludec: four times lower pharmacodynamic variability than insulin glargine under steady-state conditions in type 1 diabetes. Diabetes Obes Metab. 2012;14:859–64. [PubMed: 22594461]
- 55.
-
Ratner RE, Gough SC, Mathieu C, Del Prato S, Bode B, Mersebach H, et al. Hypoglycaemia risk with insulin degludec compared with insulin glargine in type 2 and type 1 diabetes: a pre-planned meta-analysis of phase 3 trials. Diabetes Obes Metab. 2013;15:175–84. [PMC free article: PMC3752969] [PubMed: 23130654]
- 56.
-
Marso SP, McGuire DK, Zinman B, Poulter NR, Emerson SS, Pieber TR, et al. Efficacy and Safety of Degludec versus Glargine in Type 2 Diabetes. N Engl J Med. 2017;377:723–32. [PMC free article: PMC5731244] [PubMed: 28605603]
- 57.
-
Lane W, Bailey TS, Gerety G, Gumprecht J, Philis-Tsimikas A, Hansen CT, et al. Effect of Insulin Degludec vs Insulin Glargine U100 on Hypoglycemia in Patients With Type 1 Diabetes: The SWITCH 1 Randomized Clinical Trial. JAMA. 2017;318:33–44. [PMC free article: PMC5817477] [PubMed: 28672316]
- 58.
-
Wysham C, Bhargava A, Chaykin L, de la Rosa R, Handelsman Y, Troelsen LN, et al. Effect of Insulin Degludec vs Insulin Glargine U100 on Hypoglycemia in Patients With Type 2 Diabetes: The SWITCH 2 Randomized Clinical Trial. JAMA. 2017;318:45–56. [PMC free article: PMC5817473] [PubMed: 28672317]
- 59.
-
Grunberger G. Insulin analogs-are they worth it? Yes! Diabetes Care. 2014;37:1767–70. [PubMed: 24855159]
- 60.
-
Riddle MC, Rosenstock J, Gerich J. Insulin Glargine Study I. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care. 2003;26:3080–6. [PubMed: 14578243]
- 61.
-
Vague P, Selam JL, Skeie S, De Leeuw I, Elte JW, Haahr H, et al. Insulin detemir is associated with more predictable glycemic control and reduced risk of hypoglycemia than NPH insulin in patients with type 1 diabetes on a basal-bolus regimen with premeal insulin aspart. Diabetes Care. 2003;26:590–6. [PubMed: 12610006]
- 62.
-
Riddle MC, Bolli GB, Ziemen M, Muehlen-Bartmer I, Bizet F, Home PD, et al. New insulin glargine 300 units/mL versus glargine 100 units/mL in people with type 2 diabetes using basal and mealtime insulin: glucose control and hypoglycemia in a 6-month randomized controlled trial (EDITION 1). Diabetes Care. 2014;37:2755–62. [PubMed: 25078900]
- 63.
-
Yki-Jarvinen H, Bergenstal R, Ziemen M, Wardecki M, Muehlen-Bartmer I, Boelle E, et al. New insulin glargine 300 units/mL versus glargine 100 units/mL in people with type 2 diabetes using oral agents and basal insulin: glucose control and hypoglycemia in a 6-month randomized controlled trial (EDITION 2). Diabetes Care. 2014;37:3235–43. [PubMed: 25193531]
- 64.
-
Bolli GB, Riddle MC, Bergenstal RM, Ziemen M, Sestakauskas K, Goyeau H, et al. New insulin glargine 300 U/ml compared with glargine 100 U/ml in insulin-naive people with type 2 diabetes on oral glucose-lowering drugs: a randomized controlled trial (EDITION 3). Diabetes Obes Metab. 2015;17:386–94. [PMC free article: PMC4409854] [PubMed: 25641260]
- 65.
-
Holman RR, Farmer AJ, Davies MJ, Levy JC, Darbyshire JL, Keenan JF, et al. Three-year efficacy of complex insulin regimens in type 2 diabetes. N Engl J Med. 2009;361:1736–47. [PubMed: 19850703]
- 66.
- 67.
- 68.
-
Cryer PE. Mechanisms of hypoglycemia-associated autonomic failure in diabetes. N Engl J Med. 2013;369:362–72. [PubMed: 23883381]
- 69.
-
Diabetes Control Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86. Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, et al. [PubMed: 8366922]
- 70.
-
Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837–53. [PubMed: 9742976]
- 71.
-
Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360:129–39. [PubMed: 19092145]
- 72.
-
Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545–59. Gerstein HC, Miller ME, Byington RP, Goff DC, Jr., Bigger JT, et al. [PMC free article: PMC4551392] [PubMed: 18539917]
- 73.
-
Advance Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560–72. Patel A, MacMahon S, Chalmers J, Neal B, Billot L, et al. [PubMed: 18539916]
- 74.
-
Patterson CC, Dahlquist G, Harjutsalo V, Joner G, Feltbower RG, Svensson J, et al. Early mortality in EURODIAB population-based cohorts of type 1 diabetes diagnosed in childhood since 1989. Diabetologia. 2007;50:2439–42. [PubMed: 17901942]
- 75.
- 76.
-
McCoy RG, Lipska KJ, Yao X, Ross JS, Montori VM, Shah ND. Intensive Treatment and Severe Hypoglycemia Among Adults With Type 2 Diabetes. JAMA internal medicine. 2016;176:969–78. [PMC free article: PMC5380118] [PubMed: 27273792]
- 77.
-
Desouza C, Salazar H, Cheong B, Murgo J, Fonseca V. Association of hypoglycemia and cardiac ischemia: a study based on continuous monitoring. Diabetes Care. 2003;26:1485–9. [PubMed: 12716809]
- 78.
- 79.
- 80.
-
Miller ME, Bonds DE, Gerstein HC, Seaquist ER, Bergenstal RM, Calles-Escandon J, et al. The effects of baseline characteristics, glycaemia treatment approach, and glycated haemoglobin concentration on the risk of severe hypoglycaemia: post hoc epidemiological analysis of the ACCORD study. BMJ. 2010;340:b5444. [PMC free article: PMC2803743] [PubMed: 20061360]
- 81.
-
Bremer JP, Jauch-Chara K, Hallschmid M, Schmid S, Schultes B. Hypoglycemia unawareness in older compared with middle-aged patients with type 2 diabetes. Diabetes Care. 2009;32:1513–7. [PMC free article: PMC2713637] [PubMed: 19487634]
- 82.
-
de Galan BE, Zoungas S, Chalmers J, Anderson C, Dufouil C, Pillai A, et al. Cognitive function and risks of cardiovascular disease and hypoglycaemia in patients with type 2 diabetes: the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial. Diabetologia. 2009;52:2328–36. [PubMed: 19688336]
- 83.
-
American Diabetes Association. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2018. Diabetes Care. 2018;41:S55–S64. [PubMed: 29222377]
- 84.
-
Meneghini LF, Rosenberg KH, Koenen C, Merilainen MJ, Luddeke HJ. Insulin detemir improves glycaemic control with less hypoglycaemia and no weight gain in patients with type 2 diabetes who were insulin naive or treated with NPH or insulin glargine: clinical practice experience from a German subgroup of the PREDICTIVE study. Diabetes Obes Metab. 2007;9:418–27. [PubMed: 17391170]
- 85.
-
Rosenstock J, Davies M, Home PD, Larsen J, Koenen C, Schernthaner G. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetologia. 2008;51:408–16. [PMC free article: PMC2235909] [PubMed: 18204830]
- 86.
-
Davies MJ, Derezinski T, Pedersen CB, Clauson P. Reduced weight gain with insulin detemir compared to NPH insulin is not explained by a reduction in hypoglycemia. Diabetes Technol Ther. 2008;10:273–7. [PubMed: 18715200]
- 87.
-
Buse JB, Wolffenbuttel BH, Herman WH, Hippler S, Martin SA, Jiang HH, et al. The DURAbility of Basal versus Lispro mix 75/25 insulin Efficacy (DURABLE) trial: comparing the durability of lispro mix 75/25 and glargine. Diabetes Care. 2011;34:249–55. [PMC free article: PMC3024329] [PubMed: 21270182]
- 88.
-
Radermecker RP, Scheen AJ. Allergy reactions to insulin: effects of continuous subcutaneous insulin infusion and insulin analogues. Diabetes Metab Res Rev. 2007;23:348–55. [PubMed: 17216593]
- 89.
-
Hemkens LG, Grouven U, Bender R, Gunster C, Gutschmidt S, Selke GW, et al. Risk of malignancies in patients with diabetes treated with human insulin or insulin analogues: a cohort study. Diabetologia. 2009;52:1732–44. [PMC free article: PMC2723679] [PubMed: 19565214]
- 90.
-
Jonasson JM, Ljung R, Talback M, Haglund B, Gudbjornsdottir S, Steineck G. Insulin glargine use and short-term incidence of malignancies-a population-based follow-up study in Sweden. Diabetologia. 2009;52:1745–54. [PubMed: 19588120]
- 91.
-
Colhoun HM, Group SE. Use of insulin glargine and cancer incidence in Scotland: a study from the Scottish Diabetes Research Network Epidemiology Group. Diabetologia. 2009;52:1755–65. [PMC free article: PMC2723678] [PubMed: 19603149]
- 92.
-
Rosenstock J, Fonseca V, McGill JB, Riddle M, Halle JP, Hramiak I, et al. Similar risk of malignancy with insulin glargine and neutral protamine Hagedorn (NPH) insulin in patients with type 2 diabetes: findings from a 5 year randomised, open-label study. Diabetologia. 2009;52:1971–3. [PMC free article: PMC2723677] [PubMed: 19609501]
- 93.
-
Home PD, Lagarenne P. Combined randomised controlled trial experience of malignancies in studies using insulin glargine. Diabetologia. 2009;52:2499–506. [PMC free article: PMC2776153] [PubMed: 19756478]
- 94.
-
Origin Trial Investigators. Basal insulin and cardiovascular and other outcomes in dysglycemia. N Engl J Med. 2012;367:319–28. Gerstein HC, Bosch J, Dagenais GR, Diaz R, Jung H, et al. [PubMed: 22686416]
- 95.
-
Hirsch IB. Type 1 diabetes mellitus and the use of flexible insulin regimens. Am Fam Physician 1999;60:2343-52, 55-6. [PubMed: 10593324]
- 96.
-
Low Wang CC. Medical Management of Type 1 Diabetes. In: Shah AC, ed. 7th ed. ed.
- 97.
-
Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353:2643–53. [PMC free article: PMC2637991] [PubMed: 16371630]
- 98.
-
Chiang JL, Kirkman MS, Laffel LM, Peters AL. Type 1 Diabetes Sourcebook A. Type 1 diabetes through the life span: a position statement of the American Diabetes Association. Diabetes Care. 2014;37:2034–54. [PMC free article: PMC5865481] [PubMed: 24935775]
- 99.
-
American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019;42:S90–S102. [PubMed: 30559235]
- 100.
-
Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32:193–203. [PMC free article: PMC2606813] [PubMed: 18945920]
- 101.
-
Hermann LS. Optimising therapy for insulin-treated type 2 diabetes mellitus. Drugs Aging. 2000;17:283–94. [PubMed: 11087006]
- 102.
-
DeWitt DE, Dugdale DC. Using new insulin strategies in the outpatient treatment of diabetes: clinical applications. JAMA. 2003;289:2265–9. [PubMed: 12734138]
- 103.
-
American Diabetes Association. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019;42:S61–S70. [PubMed: 30559232]
- 104.
-
Meneghini L, Atkin SL, Gough SC, Raz I, Blonde L, Shestakova M, et al. The efficacy and safety of insulin degludec given in variable once-daily dosing intervals compared with insulin glargine and insulin degludec dosed at the same time daily: a 26-week, randomized, open-label, parallel-group, treat-to-target trial in individuals with type 2 diabetes. Diabetes Care. 2013;36:858–64. [PMC free article: PMC3609505] [PubMed: 23340894]
- 105.
-
Fanelli CG, Pampanelli S, Porcellati F, Rossetti P, Brunetti P, Bolli GB. Administration of neutral protamine Hagedorn insulin at bedtime versus with dinner in type 1 diabetes mellitus to avoid nocturnal hypoglycemia and improve control. A randomized, controlled trial. Annals of internal medicine. 2002;136:504–14. [PubMed: 11926785]
- 106.
-
Francis AJ, Home PD, Hanning I, Alberti KG, Tunbridge WM. Intermediate acting insulin given at bedtime: effect on blood glucose concentrations before and after breakfast. Br Med J (Clin Res Ed). 1983;286:1173–6. [PMC free article: PMC1547399] [PubMed: 6404377]
- 107.
-
Raskin P, Bode BW, Marks JB, Hirsch IB, Weinstein RL, McGill JB, et al. Continuous subcutaneous insulin infusion and multiple daily injection therapy are equally effective in type 2 diabetes: a randomized, parallel-group, 24-week study. Diabetes Care. 2003;26:2598–603. [PubMed: 12941725]
- 108.
-
Mudaliar S, Edelman SV. Insulin therapy in type 2 diabetes. Endocrinol Metab Clin North Am. 2001;30:935–82. [PubMed: 11727406]
- 109.
-
Bode BW, Sabbah HT, Gross TM, Fredrickson LP, Davidson PC. Diabetes management in the new millennium using insulin pump therapy. Diabetes Metab Res Rev. 2002;18 Suppl 1:S14–20. [PubMed: 11921425]
- 110.
-
Bode BW, Tamborlane WV, Davidson PC. Insulin pump therapy in the 21st century. Strategies for successful use in adults, adolescents, and children with diabetes. Postgrad Med. 2002;111:69–77. [PubMed: 12040864]
- 111.
-
Pickup J, Keen H. Continuous subcutaneous insulin infusion at 25 years: evidence base for the expanding use of insulin pump therapy in type 1 diabetes. Diabetes Care. 2002;25:593–8. [PubMed: 11874953]
- 112.
-
Weaver KW, Hirsch IB. The Hybrid Closed-Loop System: Evolution and Practical Applications. Diabetes Technol Ther. 2018;20:S216–S23. [PubMed: 29873517]
- 113.
-
Blonde L, Merilainen M, Karwe V, Raskin P, Group TS. Patient-directed titration for achieving glycaemic goals using a once-daily basal insulin analogue: an assessment of two different fasting plasma glucose targets - the TITRATE study. Diabetes Obes Metab. 2009;11:623–31. [PubMed: 19515182]
- 114.
-
Holleman F, van den Brand JJ, Hoven RA, van der Linden JM, van der Tweel I, Hoekstra JB, et al. Comparison of LysB28, ProB29-human insulin analog and regular human insulin in the correction of incidental hyperglycemia. Diabetes Care. 1996;19:1426–9. [PubMed: 8941477]
- 115.
-
Kong N, Kitchen MM, Ryder RE. The use of lispro for high sugar content snacks between meals in intensive insulin regimens. Diabet Med. 2000;17:331–2. [PubMed: 10821304]
- 116.
-
Dafne Study Group. Training in flexible, intensive insulin management to enable dietary freedom in people with type 1 diabetes: dose adjustment for normal eating (DAFNE) randomised controlled trial. BMJ. 2002;325:746. [PMC free article: PMC128375] [PubMed: 12364302]
- 117.
-
Hirsch IB, Farkas-Hirsch R, Skyler JS. Intensive insulin therapy for treatment of type I diabetes. Diabetes Care. 1990;13:1265–83. [PubMed: 2276310]
- 118.
-
Miller KM, Beck RW, Bergenstal RM, Goland RS, Haller MJ, McGill JB, et al. Evidence of a strong association between frequency of self-monitoring of blood glucose and hemoglobin A1c levels in T1D exchange clinic registry participants. Diabetes Care. 2013;36:2009–14. [PMC free article: PMC3687326] [PubMed: 23378621]
- 119.
-
Stahl M, Brandslund I, Jorgensen LG, Hyltoft Petersen P, Borch-Johnsen K, de Fine Olivarius N. Can capillary whole blood glucose and venous plasma glucose measurements be used interchangeably in diagnosis of diabetes mellitus? Scand J Clin Lab Invest. 2002;62:159–66. [PubMed: 12004932]
- 120.
-
Danne T, Nimri R, Battelino T, Bergenstal RM, Close KL, DeVries JH, et al. International Consensus on Use of Continuous Glucose Monitoring. Diabetes Care. 2017;40:1631–40. [PMC free article: PMC6467165] [PubMed: 29162583]
- 121.
-
Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kroger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, non-masked, randomised controlled trial. Lancet. 2016;388:2254–63. [PubMed: 27634581]
- 122.
-
Haak T, Hanaire H, Ajjan R, Hermanns N, Riveline JP, Rayman G. Flash Glucose-Sensing Technology as a Replacement for Blood Glucose Monitoring for the Management of Insulin-Treated Type 2 Diabetes: a Multicenter, Open-Label Randomized Controlled Trial. Diabetes Ther. 2017;8:55–73. [PMC free article: PMC5306122] [PubMed: 28000140]
- 123.
-
Pickup JC, Freeman SC, Sutton AJ. Glycaemic control in type 1 diabetes during real time continuous glucose monitoring compared with self monitoring of blood glucose: meta-analysis of randomised controlled trials using individual patient data. BMJ. 2011;343:d3805. [PMC free article: PMC3131116] [PubMed: 21737469]
- 124.
-
New JP, Ajjan R, Pfeiffer AF, Freckmann G. Continuous glucose monitoring in people with diabetes: the randomized controlled Glucose Level Awareness in Diabetes Study (GLADIS). Diabet Med. 2015;32:609–17. [PubMed: 25661981]
Principles of Pharmacology for Medical Assisting 5th Edition Answer Key
Source: https://www.ncbi.nlm.nih.gov/books/NBK278938/